Vitamin K and its effects on coagulation were discovered more than 80 years ago. The Danish scientist, Henrik Dam, observed that chicks fed an extremely low fat diet for several weeks developed haemorrhages owing to the lack of an unknown factor. Dam demonstrated that a fat-soluble factor was the cause of the haemorrhages and subsequent studies revealed that it could be found in green vegetables and liver; by adding these foodstuffs to the diet, normal coagulation was obtained.
The complex enzymatic reactions involved in coagulation were not known at that time; but, they were able to demonstrate that a prothrombin fraction from chick plasma, together with the “new” factor, resulted in coagulation. Dam called the factor vitamin K as the letter “K” is derived from the German word ‘koagulation’. He was also able to isolate an oil fraction of vitamin K from alfalfa.
Several groups worked on the isolation and characterisation of vitamin K during the 1930s. During this period, phylloquinone (vitamin K1) was characterised and synthesised by a US group headed by Doisy, who identified the naphthoquinone ring structure of vitamin K1. For their contribution to the structure and the effects of vitamin K, Dam and Doisy received the Nobel Prize in 1943.
The structures of the other K vitamins (menaquinones) were not published until the late 1950s
During the next 20 years, very little research on vitamin K was published. The structures of the other K vitamins (menaquinones) were not published until the late 1950s and it was demonstrated that it was bacteria, as opposed to green vegetables, that were able to produce menaquinones with the same naphtoquinone ring as phylloquinone, but with different side chains. After the initial discovery, it took more than two decades before the exact role of vitamin K as a cofactor for post-translational protein modification was elucidated.
The role of vitamin K as a substrate for γ-glutamyl carboxylase for the post-translational modification of certain proteins (Gla-proteins) and the recycling of vitamin K through the vitamin K cycle was not revealed until the 1970s. Thus, until then, vitamin K was considered to be a coagulation protein. Only after the identification of the important Gla-proteins in certain tissues was the acknowledgement of vitamin K as an important factor for bone and cardiovascular health recognised.
Molecular structure and sources
Vitamin K is a group of closely related fat-soluble vitamins. The most important naturally occurring forms of vitamin K are phylloquinone and menaquinones, also known as vitamin K1 and vitamin K2, respectively (Figure 1). The vitamin K family shares a common naphtoquinone ring, but with different side chains. Vitamin K1 has a side chain of four isoprenoid units (same phytyl side chain as chlorophyll, with one double bond). Vitamin K2 consists of a group of menaquinones that are characterised by the length of their side chain, which can include up to 13 isoprene units.
Menaquinones are generally denoted as “MK-n” where n stands for the number of isoprene units. Menaquinone-7 (MK-7) and menaquinone-4 (MK-4) are the most important menaquinones, with seven and four isoprene units respectively. The differences in biological activity between the various forms of vitamin K result from the structure of the side chain.
Plants and algae synthesise phylloquinone. Thus, vitamin K1 is primarily found in green/leafy vegetables such as spinach, broccoli and kale. Vitamin K1 is the major dietary source of vitamin K, accounting for about 90% of total vitamin K intake. However, less than 20% of vitamin K1 in vegetables is absorbed.
MK-7 has a very long history of consumption, especially in Japan, in the fermented soybean dish natto
Menaquinones are of microbial origin and can be found in certain fermented food products such as selected cheeses, yoghurt and curd. As a natural dietary source, MK-7 has a very long history of consumption, especially in Japan, in the fermented soybean dish natto. In the northern regions of Japan, where natto is part of the traditional diet, as much as 40–50g can be consumed daily, resulting in intakes of 440–550µg/d of MK-7. Natto is believed to be the single biggest source of natural MK-7. Most other diets contain very little MK-7 and assumptions have been raised that there may be a deficiency in the general population.
Menaquinones are also produced by the intestinal microflora of the colon. But as vitamin K is mainly absorbed in the small intestine, the contribution is considered to be too limited for daily needs. Menaquinone-4 (MK-4) is not synthesised by bacteria, but can be produced in certain tissues by the conversion of vitamin K1 or menadione (vitamin K3). Dietary MK-4 originates from animal products; its contribution to the overall K requirement, however, is still questioned.
The vitamin K cycle
Vitamin K’s naphthoquinone ring is the functional part of the molecule. Vitamin K serves as a cofactor for the enzyme γ-glutamyl-carboxylase, which activates the so-called Gla-proteins. After activation, the Gla-proteins are able to bind calcium. The body stores limited amounts of vitamin K and recycles it through a process called the vitamin K cycle. Even though the vitamin is recycled, the body needs continuous intake to maintain optimal vitamin K levels.
Today, more than 15 Gla-proteins are known, including seven proteins involved in blood coagulation in the liver. Osteocalcin is a small Gla-protein (molecular weight 5.8 kDa, 49 amino acids) that’s uniquely synthesised in bone. Matrix Gla-protein, MGP, is another Gla-protein (molecular weight 10 kDa, 84 amino acids) that’s synthesised primarily by the vascular smooth muscle cells of blood vessel walls. Osteocalcin plays an important role in bone building and remodelling, whereas MGP is a strong natural inhibitor of tissue calcification. Both proteins need the vitamin K-dependent carboxylation to be fully active. In healthy subjects, all coagulation proteins are fully carboxylated. Without supplementation, only 20–30% of osteocalcin and/or MGP are in the active form. Figure 2 shows how vitamin K works together with γ-glutamyl-carboxylase to activate osteocalcin (OC) in bone, and matrix Gla-protein (MGP) in the vessel wall.
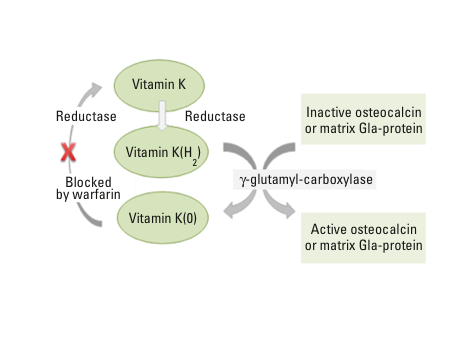
Figure 2: The vitamin K cycle; vitamin K acts as a cofactor to activate Gla-proteins. Vitamin K is recycled
Calcium metabolism
As explained above, vitamin K is a cofactor involved in the activation of Gla-proteins, making them able to bind calcium. Activated osteocalcin found in bone tissue (osteoblasts) binds calcium and ensures that calcium is incorporated into the bone. Similarly, in the vessel walls, MGP is activated by vitamin K2. MGP is the strongest known inhibitor of vessel calcification. In its active form, MGP prevents calcium deposition in the vessel walls. A high proportion of osteocalcin and MGP molecules are inactive (uncarboxylated) in blood samples from healthy subjects; many studies have documented the beneficial effects of vitamin K2 supplementation by reducing the levels of inactive Gla-proteins in blood and thereby improving bone and cardiovascular health.
Wide-ranging efficacies between K1, K2 and MK-7
Like all other fat-soluble vitamins, vitamin K is absorbed as chylomicrons (small fat particles) in the upper part of the intestine and transported by the lymphatic system to the liver. It has been demonstrated that the presence of fatty food and bile salts increases the uptake of all K vitamins. The degree of uptake is dependent on the chemical structure of the vitamin and the source.
As already mentioned, by eating vegetable such as broccoli, only 15–20% of vitamin K1 is readily taken up by the body; in its free form, a much higher proportion is absorbed. MK-7, by contrast, is efficiently taken up in the presence of fat (with a meal, for example), whereas MK-4 is poorly absorbed, even in the presence of fat.
By eating vegetable such as broccoli, only 15–20% of vitamin K1 is readily taken up by the body
A major difference between vitamin K1 (and MK-4) and MK-7 is their respective half-lives. Although they are all absorbed to varying degrees in the presence of fat, vitamin K1 (and MK-4) quickly disappears from circulation (half-life = 1–2 hours). MK-7 has a very long half-life (2–3 days). The reason for this considerable difference derives from their distribution and breakdown in the body. Vitamin K1 and MK-4 are mainly transported in the blood via triglyceride-rich lipoprotein fractions whereas MK-7 (and other long-chain menaquinones) is transported by low-density lipoproteins.
Because of the large difference in uptake and half-lives, the steady state concentration of MK-7 is substantially higher than that of vitamin K1 when subjects are given equimolar amounts (same number of molecules). As a result, MK-7 is more accessible to extrahepatic organs such as bone and vessel walls, resulting in the more efficacious carboxylation of osteocalcin and MGP. Dietary supplement tablets typically contain 50–100µg of vitamin K. Based on literature data, only vitamin K2 (MK-7) seems to be efficacious with respect to beneficial effects on bone and cardiovascular health in supplemental doses.
During the last decade, scientific data has demonstrated that vitamin K plays important roles beyond coagulation for bone and cardiovascular health.